Notice: Function Elementor\Controls_Manager::add_control_to_stack was called incorrectly. Cannot redeclare control with same name "eael_image_masking_upload_pro_message". Please see Debugging in WordPress for more information. (This message was added in version 1.0.0.) in /data/web/e44470/html/apps/wordpress-92643/wp-includes/functions.php on line 6121
Notice: Function Elementor\Controls_Manager::add_control_to_stack was called incorrectly. Cannot redeclare control with same name "eael_image_masking_upload_pro_message". Please see Debugging in WordPress for more information. (This message was added in version 1.0.0.) in /data/web/e44470/html/apps/wordpress-92643/wp-includes/functions.php on line 6121
Notice: Function Elementor\Controls_Manager::add_control_to_stack was called incorrectly. Cannot redeclare control with same name "eael_image_masking_upload_pro_message". Please see Debugging in WordPress for more information. (This message was added in version 1.0.0.) in /data/web/e44470/html/apps/wordpress-92643/wp-includes/functions.php on line 6121
Notice: Function Elementor\Controls_Manager::add_control_to_stack was called incorrectly. Cannot redeclare control with same name "eael_image_masking_upload_pro_message". Please see Debugging in WordPress for more information. (This message was added in version 1.0.0.) in /data/web/e44470/html/apps/wordpress-92643/wp-includes/functions.php on line 6121

Venous Disease Centre
Chronic venous insufficiency or CVI is a medical condition where the veins cannot pump enough blood back to the heart. It is sometimes referred to as an "impaired musculovenous pump", this is due to damaged or "incompetent" valves. Are your veins pumping out, your skin discoloured, legs swelling, feeling heavy or crampy: if your legs feel uncomfortable, get a vascular check-up. It does not hurt.

Centre for Proctology
The Clinic together with Consultants from the Vienna University Clinic offers advanced diagnostic and therapeutic services including robotic colorectal surgery for disorders of the colon, rectum, anus and pelvic floor within a friendly and reassuring environment. The Rapid Access Proctology Clinic reduces waiting time and improve public and professional awareness of the need for early detection and treatment of colorectal lesions
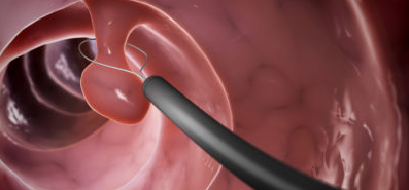

Endoscopy Centre
The Endoscopy Centre performs a comprehensive range of endoscopic procedures that allow both diagnosis and treatment of gastrointestinal disorders, such as peptic ulcers, polyps, inflammation and tumors. It is professionally committed to ensuring that your experience with us is relaxed and worry-free, from consultation through recovery. To assist us in achieving a mutual satisfactory procedure, we ask that you read our guidelines.
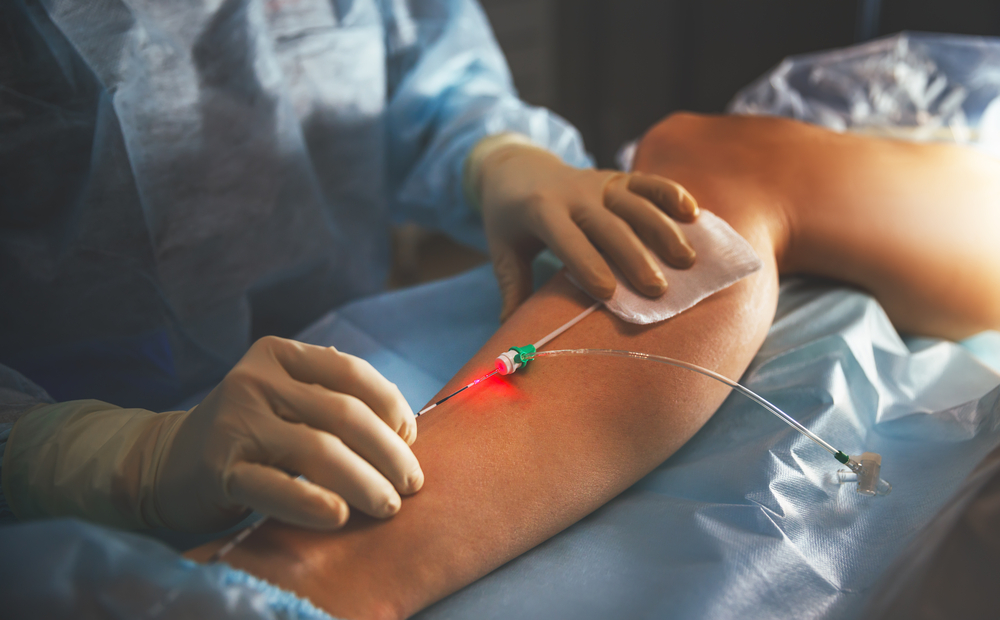
Endovenous Laser Treatment
Endovenous laser treatment is a procedure to treat larger varicose veins in the legs. A laser fibre is passed through a thin tube (catheter) into the vein. While doing this, the doctor watches the vein on a duplex ultrasound screen. Laser is less painful than vein ligation and stripping, and it has a shorter recovery time. Only local diluted anaesthesia is needed with mild sedation for this laser treatment.
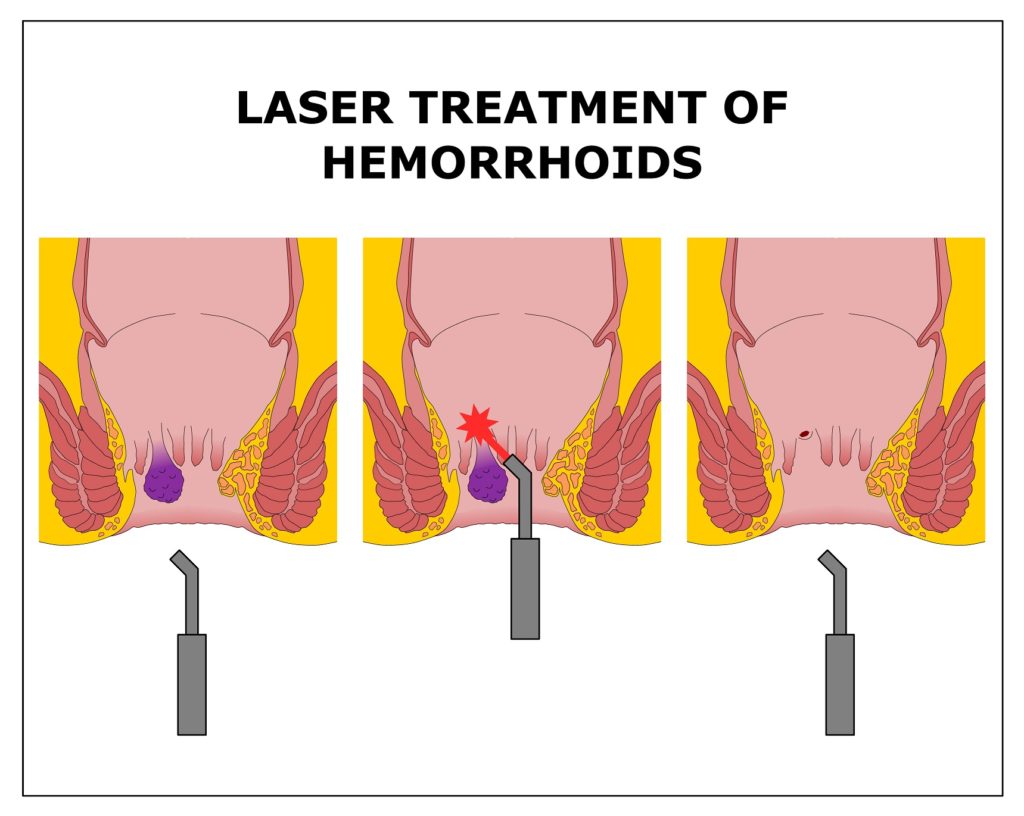
Laser-assisted Haemorrhoidectomy
The Clinic offers the newest laser technology for surgical treatment assisted with Duplex sonography for internal haemorrhoids. The procedure permits a smoother, less painful and faster recovery. The affected area is treated with pinpoited laser energy to the affected haemorrhoid and the problem is solved within a few minutes. Patients can resume their normal lives immediately after surgery.
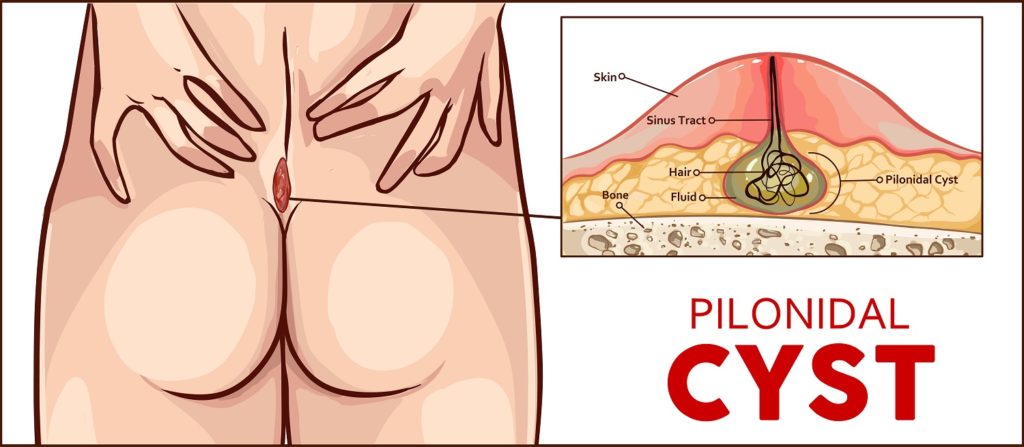
Pit Picking and Laser-assisted sinusectomy
The Endoscopy Center is professionally committed to ensuring that your experience with us is relaxed and worry-free, from consultation through recovery. To assist us, we ask that you read and comply with all our guidelines. Endoscopic laser-assisted sinusectomy shows a low recurrence rate and marsupilisation of the wound a prompt healing. Following this procedure patients can return to work shortly afterwards. Mild discomfort while the procedure is performed in local analgesia is corrected with light sedation and with over the counter pain killers in the immediate postoperative period.

The Sievering Clinic
The Sievering Clinic is situated in the heart of the private medical services in Vienna with Rudolfiner Hospital just across the street. It is a surgical outpatient clinic offering state-of-art diagnosis and treatments for the fields of phlebology (diagnosis and treatment of vascular disease), proctology (diseases of the rectum) and gastrointestinal diseases.


City Clinic in Heiligenkreuzerhof
You can also visit us at our private clinic in the centre of the city. Heiligenkreuzerhof offers great access just a few minutes from St Stephen and sufficient parking area at Schwedenplatz. Walking distance from the U1 Stephanplatz and U1 U4 Schwedenplatz